
Download
Original Article
Investigating the synergistic and modulatory effects of cannabidiol with levodopa and dietary protein in Parkinson’s disease
Wajid Rahim Awan1, Afia Zia1*, Adnan Khan2, Niamat Ullah3, Ammena Y. Binsaleh4, Nawal Al-Hoshani5, Abdullah A. Alqasem6, Reham M. Mashat7, Ibrahim Faisal Halawani8, Majid Alhomrani8
1Department of Agricultural Chemistry and Biochemistry, The University of Agriculture, Peshawar, Pakistan;
2Department of Neurology, Lady Reading Hospital, Peshawar, Pakistan;
3Department of Human Nutrition, The University of Agriculture, Peshawar, Pakistan;
4Department of Pharmacy Practice, College of Pharmacy, Princess Nourah bint Abdulrahman University, P.O. Box 84428, Riyadh 11671, Saudi Arabia;
5Department of Biology, College of Science, Princess Nourah bint Abdulrahman University, P.O. Box 84428, Riyadh 11671, Saudi Arabia;
6Department of Medical Laboratory, College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University, Al-Kharj 11942, Saudi Arabia;
7Nutrition and Food Sciences, College of Science , King Khalid University, Abha 62529, Saudi Arabia;
8Department of Clinical Laboratory Sciences, Collage of Applied Medical Sciences, Taif University, P.O. Box 11099, Taif 21944, Saudi Arabia
Abstract
Parkinson’s disease (PD) is a complex neurodegenerative disorder primarily managed with levodopa, which, despite its efficacy, is limited by long-term complications and dietary interactions. An 8-week randomized clinical trial (n = 96) was designed to assess cannabidiol (CBD) as an adjunct to levodopa, examining the efficacy of dietary protein intake. Participants were assigned to either levodopa monotherapy or levodopa plus CBD (300 mg/day) and further stratified based on dietary protein control. Symptom severity was assessed using the Unified Parkinson’s Disease Rating Scale (UPDRS). The CBD group demonstrated a significantly greater improvement in total UPDRS scores (mean reduction: 51.2 ± 4.5) compared to the levodopa-only group (36.4 ± 3.2). Within the CBD group, patients following a protein-controlled diet showed enhanced improvement (53.6 ± 4.1) compared to those without dietary control (48.9 ± 4.8; P < 0.05). Improvements were observed across motor (tremor, rigidity, bradykinesia) and nonmotor (depression, motivation, sleep) domains. CBD was well-tolerated, with only mild, transient side effects such as drowsiness and dry mouth. These findings suggest that CBD is a safe and effective adjunctive therapy for PD, capable of enhancing both motor and nonmotor symptom control. Additionally, the study also indicated that dietary protein management can influence therapeutic outcomes, underscoring the importance of integrated pharmacological and nutritional strategies in PD management. This study recommends a large-scale study to explore underlying mechanisms.
Key words: adjunctive therapy, cannabidiol (CBD), dietary protein, levodopa, neurodegenerative disorder, randomized clinical trial (RCT), UPDRS
*Corresponding Author: Afia Zia, Department of Agricultural Chemistry and Biochemistry, The University of Agriculture, Peshawar, Pakistan. Email: [email protected]
Academic Editor: Prof. Tommaso Beccari – University of Perugia, Italy
Received: 8 July 2025; Accepted: 5 August 2025; Published: 1 October 2025
© 2025 Codon Publications
This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY-NC-SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/)
Introduction
Parkinson’s disease (PD) stands as the fastest-growing chronic neurodegenerative disorder that primarily affects the motor system but also encompasses a wide spectrum of nonmotor symptoms (Hodgson et al., 2025; Rana et al., 2015; Rinaldi, 2025). It is currently the second most prevalent neurodegenerative condition globally, with a rising incidence linked to aging populations (Ben-Shlomo et al., 2024; Grotewold and Albin, 2024; Peña-Zelayeta et al., 2025). It is a rising global health challenge affecting nearly 10 million people, with cases projected to double by 2040 (Su et al., 2025). Pathologically, PD is characterized by the gradual degeneration of dopaminergic neurons in the substantia nigra pars compacta, resulting in striatal dopamine depletion. This neurochemical deficit manifests clinically as classic motor symptoms, including resting tremor, rigidity, bradykinesia, and postural instability. Moreover, patients often experience nonmotor symptoms such as depression, anxiety, sleep disturbances, fatigue, constipation, and cognitive impairment, all of which substantially diminish the quality of life and complicate disease management (Dalla Verde et al., 2025; Ferrer, 2011; Jiang et al., 2025; Kumar et al., 2024; Schneider and Obeso, 2014).
To treat PD, levodopa (L-DOPA) is usually coadministered with a peripheral decarboxylase inhibitor (e.g., carbidopa as in Sinemet) (Ajagun et al., 2024; Müller et al., 2024). This has remained one of the key standards for symptomatic treatment of PD. Levodopa therapy effectively alleviates motor symptoms, particularly in early stages of the disease (Khor and Hsu, 2007; Müller, 2020, 2025; Riederer et al., 2025; Tambasco et al., 2018; Teil et al., 2025). However, with long-term use, motor complications such as motor fluctuations, on–off phenomena, and levodopa-induced dyskinesias (LID) become increasingly common. Moreover, the narrow therapeutic gap of levodopa and its variable absorption influenced by factors such as gastric emptying and dietary protein intake pose substantial clinical challenges. Specifically, dietary proteins containing large neutral amino acids (LNAAs) compete with levodopa for active transport across the blood–brain barrier, thereby reducing its bioavailability and therapeutic efficacy (Nord, 2017; Rusch et al., 2023). This interaction underscores the need to explore adjunctive therapies that either enhance levodopa’s effectiveness or offer independent symptomatic relief. Several adjunct therapies, such as dopamine agonists (e.g., pramipexole), MAO-B inhibitors (e.g., rasagiline), and NMDA antagonists (e.g., amantadine), have been investigated to address levodopa-induced complications. However, their benefits are often offset by dose-limiting side effects like hallucinations, nausea, and impulse control disorders (Müller et al., 2024; Tambasco et al., 2018). In contrast, cannabidiol (CBD), a nonpsychoactive phytocannabinoid, has emerged as a promising candidate due to its favorable safety profile and multitarget mechanism involving the endocannabinoid system and serotonergic signaling (Bhunia et al., 2022; Del-Bel et al., 2024).
In addition to standard pharmacological approaches such as dopamine agonists (e.g., pramipexole), MAO-B inhibitors (e.g., rasagiline), and NMDA antagonists (e.g., amantadine), recent investigations have turned toward phytochemicals like CBD due to their multimodal neuroprotective potential (Bhunia et al., 2022; Riederer et al., 2025). Compared to these conventional therapies, CBD may offer broader benefits by targeting both motor and nonmotor domains while avoiding some dopaminergic side effects. In recent years, CBD, which is a nonpsychoactive phyto-cannabinoid derived from Cannabis sativa, has gained significant attention as a potential adjunct in the treatment of neurodegenerative diseases, including PD. Unlike Δ9-tetrahydrocannabinol (THC), CBD lacks euphoric or psychoactive effects, making it an attractive candidate for long-term use. Preclinical and clinical research has demonstrated that CBD exerts a broad spectrum of neuroprotective, anti-inflammatory, antioxidant, and anxiolytic effects. These effects are largely mediated through the modulation of the endocannabinoid system (ECS), involving CB1 and CB2 receptors, as well as interactions with noncannabinoid targets such as 5-HT1A serotonin receptors, TRPV1 ion channels, and PPAR-γ nuclear receptors. Collectively, these interactions influence neurotransmitter release, neuroinflammation, mitochondrial function, and cellular stress responses, all of which are relevant to PD pathophysiology (Del-Bel et al., 2024; Omotayo et al., 2024; Suryadevara et al., 2017; Vimal et al., 2023).
Furthermore, CBD has shown promise in alleviating nonmotor symptoms of PD, which are often inadequately managed with standard dopaminergic therapies. For example, studies have reported improvements in sleep quality, psychological well-being, and neurocognitive function in PD patients receiving CBD (Belgers et al., 2023; Chagas et al., 2014). In addition to symptomatic relief, there is emerging interest in CBD’s potential to modify disease progression by mitigating neurodegenerative processes such as oxidative stress, excitotoxicity, and α-synuclein aggregation hallmarks of PD neuropathology (Behl et al., 2020; Bhunia et al., 2022). A recent meta-analysis by Belgers et al. (2023) and clinical observations by Del-Bel et al. (2024) confirmed that CBD not only improves UPDRS scores in PD but also enhances sleep and mood outcomes more consistently than placebo or THC-dominant formulations. This supports its inclusion as a multitarget adjunct therapy. Recent meta-analyses and exploratory trials have shown that CBD not only improves quality of life and sleep in PD patients but may also reduce levodopa-induced dyskinesias and anxiety-related symptoms more effectively than placebo (Belgers et al., 2023; Chagas et al., 2014; Del-Bel et al., 2024).
Despite growing enthusiasm, the integration of CBD into standard PD management remains limited by gaps in clinical data, particularly regarding its efficacy when used concurrently with levodopa and its interaction with dietary factors such as protein intake. Given that both levodopa and CBD undergo hepatic metabolism (primarily via the cytochrome P450 system), potential pharmacokinetic interactions may arise, further influencing therapeutic outcomes. Moreover, while the protein redistribution diet (PRD) has been explored in optimizing levodopa pharmacodynamics, its role in modulating CBD’s bioavailability and efficacy remains poorly understood (Rusch et al., 2023). Despite these promising findings, there remains a significant gap in controlled clinical data evaluating the synergistic interaction between CBD and levodopa, especially under dietary protein-controlled conditions. No study to date has comprehensively examined this triad in Parkinson’s patients in a developing-country setting, highlighting the novelty and necessity of the present work. Therefore, the present study was designed to address these gaps by evaluating the therapeutic potential of CBD as an adjunct to Sinemet (levodopa/carbidopa) in individuals with idiopathic PD. This study primarily investigates the therapeutic impact of CBD coadministered with levodopa (Sinemet) on both motor and nonmotor symptoms in PD.
Materials and Methods
Cannabidiol preparation and preliminary treatment
To prepare CBD extract, the protocol outlined by Peres et al. (2018) with modifications from Flores-Sanchez and Verpoorte (2008) was followed. Approximately 10.5 kg of dried industrial hemp (C. sativa L.) biomass was procured. The sample was high in CBD and low in THC content (<0.3%). The biomass was processed at the Pilot Plant Unit at the Pakistan Council of Scientific and Industrial Research (PCSIR). The hemp was first manually shredded and air-dried in a controlled environment at 40°C to maintain cannabinoid integrity. After reaching a moisture content below 10%, the dried material was finely milled and sieved to mesh # 40, ensuring a consistent particle size for optimal extraction performance. Before extraction, the milled hemp was subjected to decarboxylation at 110°C for 60 min in a convection oven to convert cannabidiolic acid (CBDA) to its active neutral form, CBD.
Supercritical CO2 extraction
The extraction was carried out using a supercritical CO2 (SC–CO2) extraction unit (Model SCFE-220-40-20L, Careddi Technologies, China), following parameters optimized from Kammerer et al. (2022) and Wang et al. (2021). A total of 2.5 kg of decarboxylated hemp powder was packed into the stainless steel extraction chamber. The vessel was sealed, followed by gradual heating to 50°C. Supercritical CO2 was pumped into the vessel at a pressure of 32 MPa, well within the supercritical phase. During the extraction process, ethanol (10% w/w of CO2) was used as a cosolvent to increase CBD solubility and extraction efficiency. CO2 was maintained at a flow rate of 5 kg/h, and ethanol at 1 kg/h. The mixture was circulated through the hemp matrix for 3 h, after which the process was stopped upon stabilization of extract yield. The CBD-rich effluent was collected in a separation vessel where pressure was reduced to atmospheric levels, leading to the precipitation of cannabinoids and evaporation of CO2.
Post-extraction processing
The collected crude extract was transferred to a round-bottom flask. Rotary evaporation was performed at 40°C under 150 mbar vacuum pressure and 120 rpm rotation speed to remove residual ethanol. The process continued for 45–60 min until a viscous, amber-colored, CBD-rich extract was obtained. Final yield was measured by subtracting the flask’s pre- and post-weights.
Winterization of crude cannabis extract
Winterization was used to remove lipids and waxes from the raw cannabis extract. The crude oil was mixed with food-grade ethanol at a ratio of 10 mL of ethanol for every gram of extract. For 600 g of crude oil, approximately 6 L of ethanol was used. To ensure complete dissolution, the ethanol was preheated to about 40°C, resulting in a uniform dark solution as described by Wang et al. (2017). The solution was then stored at −80°C for 2 h to allow wax precipitation. Optimal precipitation occurred within 2 h at −80°C or 48 h at −20°C, as noted by Hazekamp (2008). Vacuum filtration was performed while the solution remained cold, initially using coarse filters (20–50 µm) followed by fine filters (5 µm), for efficient wax removal. Rotary evaporation at approximately 40°C under vacuum was then used to concentrate the winterized solution, remove ethanol to purified winterized oil, and confirm the removal of waxes, as reported by De Meijer (2009).
Quantification
Analytical quantification of CBD was performed using Gas Chromatography–Mass Spectrometry (GC-MS), following derivatization with N,O-Bis(trimethylsilyl)trifluoroacetamide (BSTFA) + 1% TMCS.
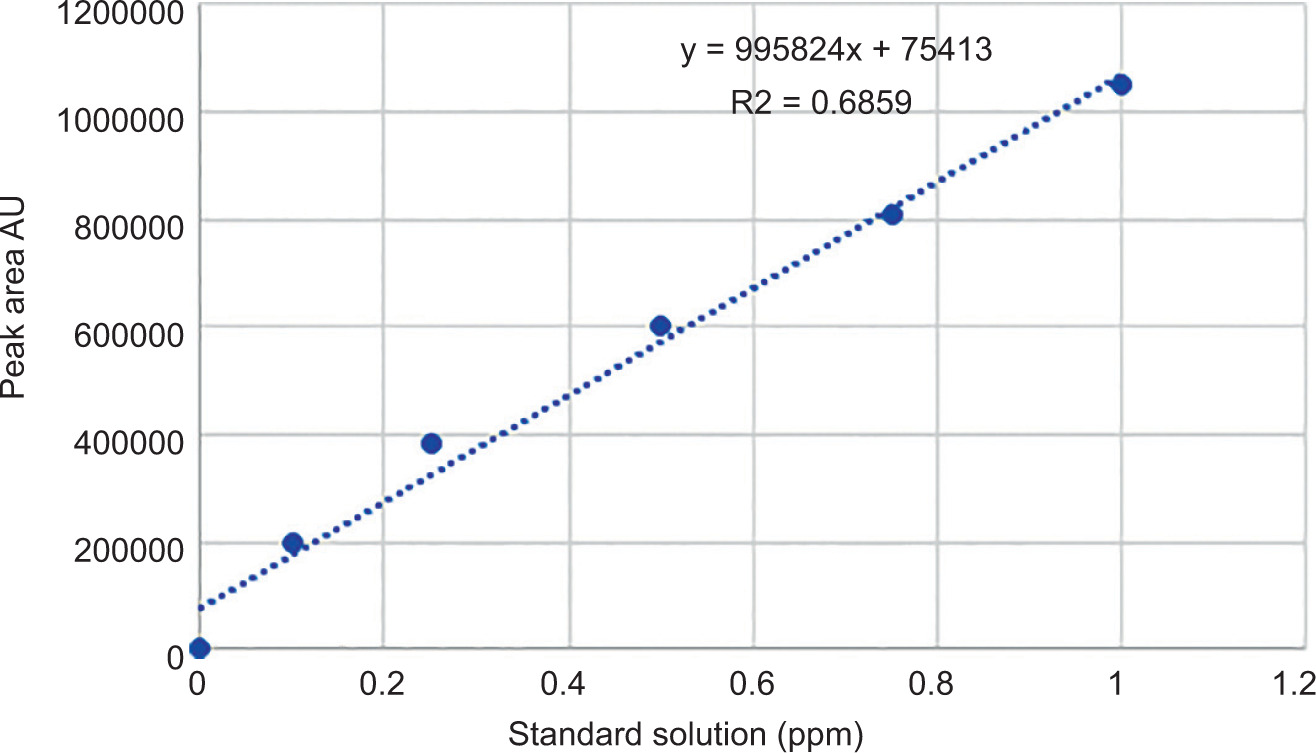
A stock solution of CBD was prepared by dissolving 10 mg of pure CBD reference standard (≥99%, Sigma-Aldrich) in 10 mL of HPLC-grade methanol, yielding a concentration of 1.0 mg/mL. Serial dilutions were prepared to obtain standard solutions in the range of 0.1–1.0 µg/mL.
Samples and standards were derivatized at 70°C for 30 min. GC-MS analysis was carried out using a Shimadzu GC-MS-QP2010 system equipped with a 5975C mass detector and an HP-5MS capillary column. The injector temperature was 280°C, and helium was used as the carrier gas at a flow rate of 1.0 mL/min. The oven was programed as initial temperature 100°C (held for 1 min), ramped to 280°C at 10°C/min, and held for 5 min. Figure 1 illustrates the calibration curve used for CBD quantification.
Figure 1. Standard curve of CBD standards.
Clinical trial design
Participants
Patients diagnosed with idiopathic PD within the last 2–4 years were recruited from neurology departments in Peshawar. Participants had stable disease conditions and were on consistent Sinemet therapy. Exclusion criteria included atypical parkinsonism, severe psychiatric illness, cognitive impairment, or inability to adhere to protocol. Ethical approval was secured (Appendix-A), and informed consent was obtained from all participants.
A total of 96 patients were enrolled and divided into two primary groups:
-
Group A (n = 24): Sinemet alone
-
Group B (n = 24): Sinemet + CBD (administered at 300 mg/day; 150 mg twice daily)
Intervention strategy
Participants received their assigned treatments over 8 weeks. Each treatment group was further subdivided into:
-
Subgroup 1 (n = 24): With protein control – Patients consumed high-protein meals (controlled) only in the evening to minimize competition with levodopa for transport across the blood–brain barrier.
-
Subgroup 2 (n = 24): Without protein control – Patients continued their habitual dietary practices without any modification in protein timing.
This design enabled evaluation of the individual and interactive effects of CBD and dietary protein on PD symptom management.
Clinical assessment
To assess treatment efficacy, the Unified Parkinson’s Disease Rating Scale (UPDRS) was administered by trained clinicians who were blinded to the treatment assignments. Assessments were conducted at baseline and post-intervention (8 weeks). Both motor and nonmotor symptoms were scored. Throughout the study, patient diaries, monthly check-ins, and adherence monitoring were used to record compliance and any side effects related to CBD intake.
Clinical assessments were conducted at baseline (Day 0) and at the end of the 8-week intervention period (Day 56). The primary outcome measure was the change in PD symptom severity, meticulously evaluated using the UPDRS parts I (Nonmotor experiences of daily living), II (Motor experiences of daily living), and III (Motor examination). Experienced neurologists, blinded to group allocation, administered all UPDRS assessments to minimize observer bias. Additionally, patient-reported outcomes were captured, including assessment of quality of life and perceived symptom changes, though detailed analysis of these may be beyond the scope of this focused paper. Safety and tolerability were rigorously monitored throughout the study, with all adverse events (AEs) reported by participants or observed by clinicians being recorded. Blood samples were collected at baseline and endpoint for routine biochemistry and hematology analyses to monitor systemic health and potential treatment-related side effects.
Statistical analysis
Data analysis was performed using SPSS (v20) and Statistix 8.1. For between-group comparisons of treatment effects, a two-factorial analysis of variance (ANOVA) was conducted using Statistix 8.1 software. This approach evaluated the statistical significance of differences among various treatment conditions, accounting for interactions between multiple factors. A significant threshold of P < 0.05 was used to determine meaningful improvements.
Results and Discussion
Cannabidiol extraction and characterization
During the current study, CBD was extracted successfully from industrial hemp biomass using supercritical carbon dioxide (SC-CO2) technology. A predecarboxylation step at 110°C was employed to convert the inactive CBDA into its active neutral form. A yield of 13.53% (w/w) was noted upon confirmation by GC-MS analysis. The cannabinoid-rich extract was further concentrated via rotary evaporation, which removed residual ethanol under controlled vacuum and temperature conditions, yielding a dense amber-colored oil. Table 1 shows all the findings related to the CBD extraction and characterization process.
Table 1. Mass balance and CBD extraction from hemp biomass.
| Material | Mass (g) | % of dried biomass (2.5 kg) |
|---|---|---|
| Fresh hemp biomass (70% moisture) | 8300 | – |
| Water removed during drying | ~5800 | – |
| Dried hemp biomass (after drying) | 2500 | 100% |
| Decarboxylated biomass (approx.) | 2490 | 99.6% (loss ~0.4%) |
| Crude extract (after extraction) | 450 | 18.0% |
| Spent biomass (extracted plant) | 2040 | 81.6% |
| Waxes removed (winterization) | 60 | 2.4% |
| Winterized hemp oil (total) | 390 | 15.6% |
| CBD content in Winterized oil | 338.25 | 13.53% |
| Other components in oil | ~51.8 | ~2.07% |
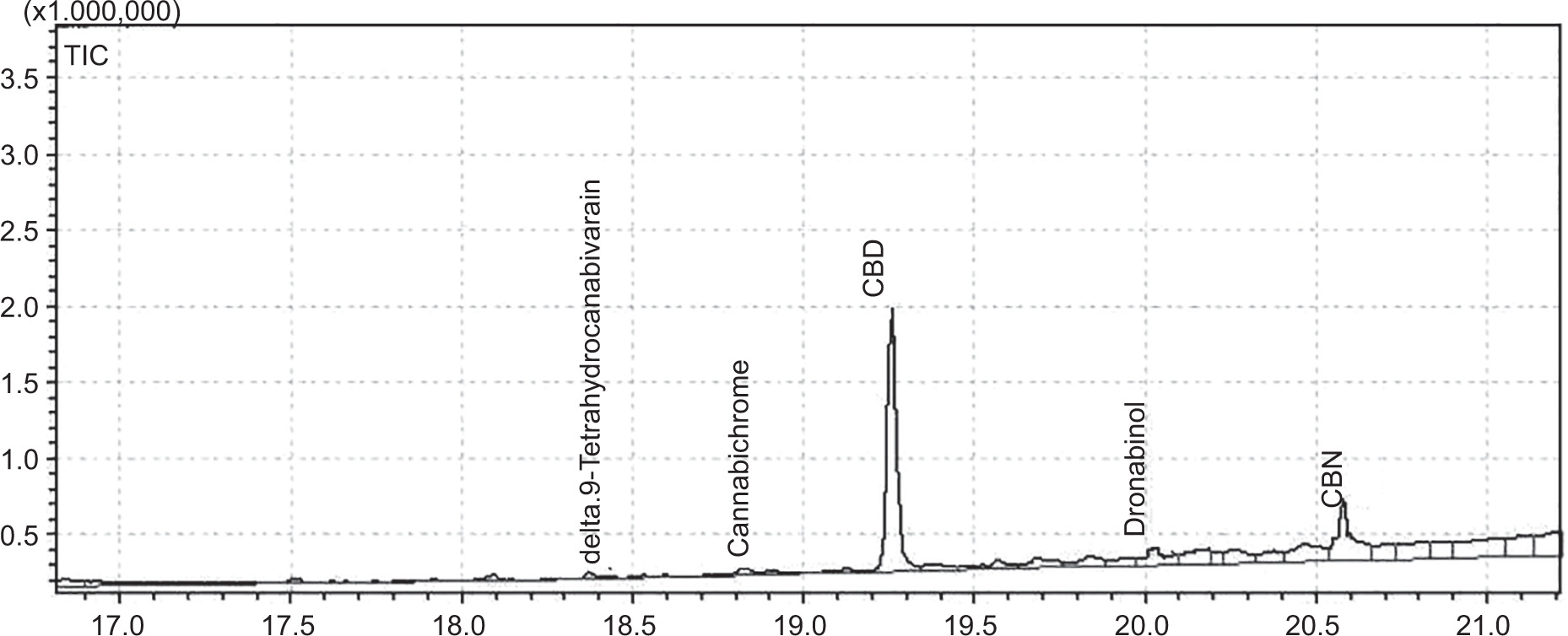
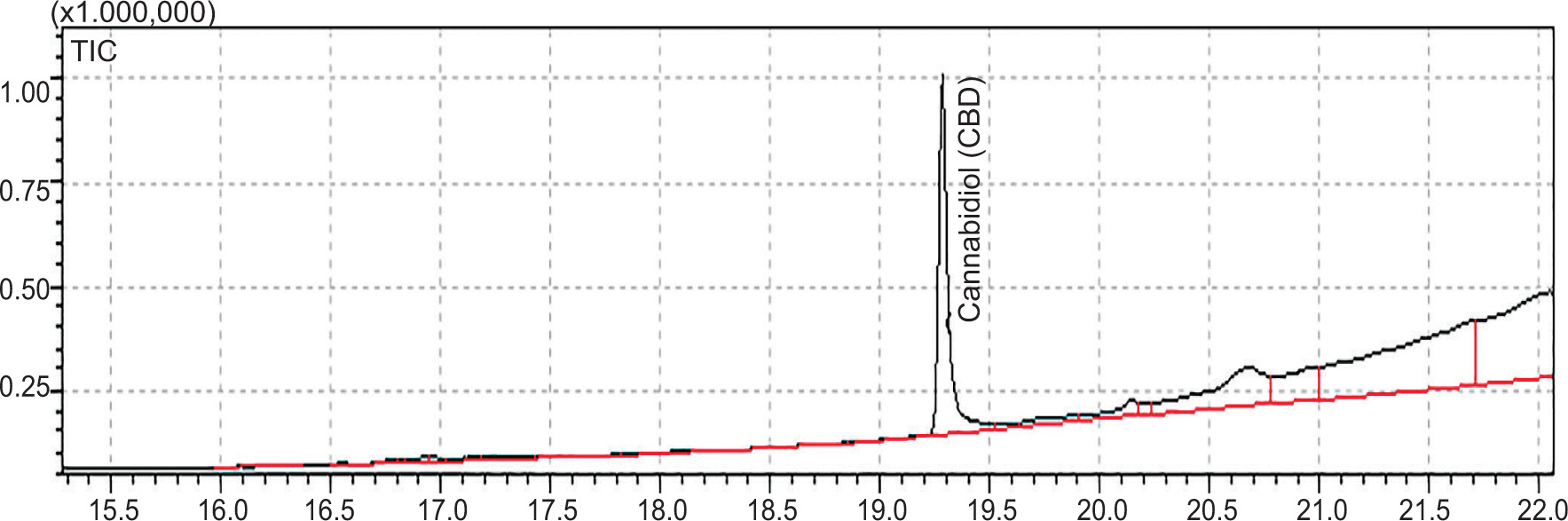
The use of ethanol as a cosolvent proved critical in increasing extraction yield by disrupting cellular matrices and enhancing the solvating power of CO2, especially for lipophilic compounds such as CBD. The sample chromatograms showed well-resolved peaks corresponding to the CBD standard, indicating high purity and accuracy of quantification (Figures 2 and 3). Based on the yield obtained, approximately 2.22 g of this extract was required to deliver a 300 mg daily dose of CBD, a quantity deemed both pharmacologically effective and clinically tolerable in PD management. This precise quantification and standardization allowed for uniform dosing across all participants, ensuring the reliability and reproducibility of the clinical outcomes.
Figure 2. Chromatogram of the sample methanolic extract.
Figure 3. Chromatogram of CBD standard.
Quantification
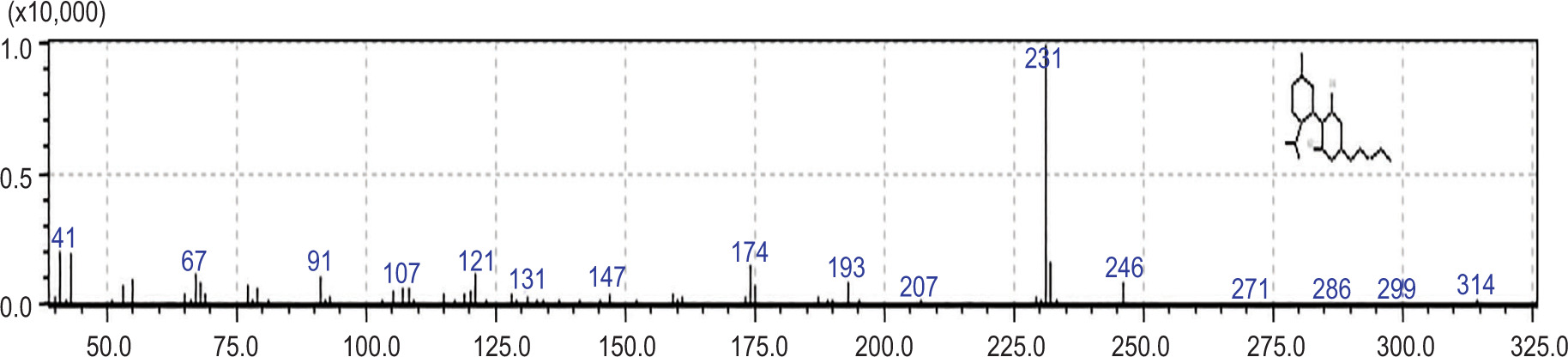
The GC-MS results confirmed the presence of CBD in the sample. This was done by matching its retention time and characteristic fragmentation pattern with standards. The GC-MS findings are shown in Figure 4. The elution of CBD at a consistent retention time and diagnostic ions at m/z 231 and 246 reflects a cleavage at the pentyl side chain and aromatic moiety, respectively. The findings were similar to those of Alonso et al. (2020). Additionally, the absence of interfering signals confirms the CBD and demonstrates the method’s specificity and reliability in complex plant matrices.
Figure 4. Entry: 109238 Library: NIST05:LIB. Formula: C21H30O2 CAS:521-37-9 MolWeight:314 RetIndex:2604. Resorcinol, 2-p-mentha-1,8-dien-3-yl-5-pentyl, (H, E) $$ 1,3-Benzenediol, 2-(3-methyl-6-(1-methylethenyl)-2-cyclohexen-1-yl)-5-pentyl $$ (1R-trans)-Cannabidiol.
Clinical efficacy of cannabidiol: Changes in UPDRS scores
The administration of CBD as an adjunct to levodopa (Sinemet) therapy led to a significant improvement in both motor and nonmotor symptoms among patients diagnosed with idiopathic Parkinson’s disease. This improvement was objectively measured using the UPDRS, a gold standard clinical tool. The baseline UPDRS scores were comparable between the Sinemet-only control group and the Sinemet + CBD intervention group. However, a mean improvement of 51.2 ± 4.5 points was observed when the patients were treated with the Sinemet + CBD group, compared to the control group, which showed only an average gain of 36.4 ± 3.2 points. This marked difference in mean scores underscores the potential of CBD in significantly enhancing therapeutic outcomes when used as a complementary intervention.
The therapeutic benefits of CBD extend across a wide range of symptoms. On the motor side, participants reported a substantial reduction in tremor intensity, muscular rigidity, bradykinesia, and difficulties with gait and posture. On the nonmotor front, there were clinically significant improvements in symptoms such as sleep disturbances, sensory complaints, depression, and anxiety, areas where conventional levodopa therapy often falls short. The multifaceted interaction of CBD with the endocannabinoid system (ECS), including CB1, CB2, and serotonin (5-HT1A) receptors, may account for its broad therapeutic profile. This finding reinforces the notion that CBD not only complements dopaminergic therapy but also independently addresses pathophysiological components of PD that are beyond the dopaminergic deficit. The significant improvements across both motor and nonmotor symptoms observed in the Sinemet + CBD group (Tables 2–4) are consistent with the multifaceted pharmacological profile of CBD. While levodopa primarily addresses dopaminergic deficits, CBD’s therapeutic breadth likely stems from its diverse interactions with the ECS and other non-ECS targets. For instance, the reported anxiolytic and antidepressant effects of CBD, which may contribute to the improvements in nonmotor symptoms like mood and motivation (Table 4), are often linked to its modulation of serotonin 5-HT1A receptors. Furthermore, its anti-inflammatory and antioxidant properties are crucial in mitigating neuroinflammation and oxidative stress, key pathological hallmarks of PD, thereby potentially contributing to improvements in motor symptoms by supporting neuronal integrity and function. The reduction in levodopa-induced dyskinesias, though not a primary outcome, may be related to CBD’s indirect modulation of cannabinoid receptors (CB1 and CB2) in the basal ganglia, which are implicated in motor control and dyskinesia pathophysiology. This broad symptomatic improvement suggests that CBD acts via distinct yet complementary pathways to levodopa, offering a more holistic approach to PD management.
Table 2. Comparative scoring of UPDRS.
| Treatment group | Baseline score | Post-treatment score | Mean improvement (±SD) |
|---|---|---|---|
| Sinemet only | 92.3 | 55.9 | 36.4 ± 3.2 |
| Sinemet + CBD | 94.6 | 43.4 | 51.2 ± 4.5 |
Table 3. The top five improved symptoms in the Sinemet-only control group based on the average UPDRS score improvement.
| Rank | Symptom | Average improvement |
|---|---|---|
| 1 | Gait | 1.33 |
| 2 | Action or postural tremor of the right hand | 1.25 |
| 3 | Body bradykinesia and hypokinesia | 1.25 |
| 4 | Tremor | 1.21 |
| 5 | Neck rigidity | 1.17 |
Table 4. The top five improved symptoms in the Sinemet + CBD group, based on the average UPDRS score improvement.
| Rank | Symptom | Average mean improvement |
|---|---|---|
| 1 | Tremor | 1.79 |
| 2 | Rigidity of left hand | 1.79 |
| 3 | Body bradykinesia and hypokinesia | 1.75 |
| 4 | Depression | 1.67 |
| 5 | Motivation/initiative | 1.63 |
Effect of dietary protein timing on CBD efficacy
While dietary protein intake is known to interfere with levodopa’s absorption due to competitive inhibition via large neutral amino acid transporters, the interaction between CBD and protein remains less well characterized. However, the current study revealed that a moderate interaction may exist. Patients receiving CBD alongside protein-controlled diets (i.e., evening-only high-protein meals) demonstrated a slightly greater improvement in UPDRS scores (53.6 ± 4.1) compared to those who continued with unrestricted protein intake (48.9 ± 4.8). Though the magnitude of difference was modest, the interaction reached statistical significance (P < 0.05), suggesting that structured protein timing may support optimal CBD efficacy, potentially by modulating gastrointestinal absorption or hepatic metabolism.
This finding is clinically relevant, especially given the increasing interest in nutrition-based modulation of pharmacotherapy. While CBD’s absorption is not as protein-sensitive as levodopa’s, the observed enhancement suggests a potential role of protein redistribution diets (PRD) even in non-levodopa-based therapies. These results warrant further pharmacokinetic investigations to determine the exact mechanisms underlying this interaction.
The observed subtle yet statistically significant modulation of CBD’s efficacy by dietary protein intake, as evidenced by differences in UPDRS gain between protein-controlled subgroups (Table 5), warrants deeper consideration. While the precise mechanisms underpinning this interaction require further investigation, existing literature on levodopa’s absorption provides a crucial framework. Levodopa, an amino acid, competes with dietary large neutral amino acids (LNAAs) for transport across the intestinal barrier and the blood–brain barrier via the L-type amino acid transporter 1 (LAT1). A high-protein meal can lead to increased plasma LNAA concentrations, subsequently reducing levodopa’s systemic availability and central nervous system uptake. Although CBD is not an amino acid, its absorption and metabolism could theoretically be influenced by the gut environment, which is significantly altered by macronutrient intake. For instance, changes in gastric emptying time or bile acid secretion due to protein consumption might indirectly affect CBD’s dissolution, absorption kinetics, or first-pass metabolism. This finding underscores the complex interplay between pharmacotherapy and nutritional factors in PD management, suggesting a pathway for personalized dietary strategies to potentially optimize the therapeutic window of both levodopa and adjunctive CBD.
Table 5. Mean UPDRS gain among the two subgroups.
| Group | Protein control | Mean UPDRS gain ± SD |
|---|---|---|
| Sinemet + CBD | No | 48.9 ± 4.8 |
| Sinemet + CBD | Yes | 53.6 ± 4.1 |
Table 6. The top five improved symptoms in the Sinemet + protein group based on average improvement.
| Rank | Symptom | Average improvement |
|---|---|---|
| 1 | Tremor | 1.54 |
| 2 | Gait | 1.50 |
| 3 | Finger taps right hand | 1.42 |
| 4 | Rigidity right hand | 1.38 |
| 5 | Rapid alternating movement of right hand | 1.38 |
Table 7. The top five most improved symptoms in the Sinemet + CBD with protein group based on UPDRS score enhancement.
| Rank | Symptom | Average improvement |
|---|---|---|
| 1 | Body bradykinesia and hypokinesia | 1.96 |
| 2 | Tremor | 1.96 |
| 3 | Rigidity of left hand | 1.88 |
| 4 | Walking and balance | 1.88 |
| 5 | Depression | 1.83 |
Table 8. Side effects observed during the clinical trial.
| Side effect | Frequency (%) |
|---|---|
| Drowsiness | 6.7 |
| Dry mouth | 5 |
| GI discomfort | 3.3 |
| Serious adverse events | 0 |
Safety profile and tolerability of cannabidiol
Over the 8-week clinical intervention, CBD demonstrated a favorable safety profile, with no serious adverse events recorded across the treatment cohort. Mild side effects were reported in a small subset of patients, with the most common being drowsiness (6.7%), dry mouth (5%), and occasional gastrointestinal discomfort (3.3%). These effects were transient and did not necessitate discontinuation of treatment. Notably, there were no reported cases of psychiatric symptoms, hallucinations, or worsening of motor fluctuations—side effects occasionally seen with dopaminergic therapy or psychoactive cannabinoids like THC. This affirms CBD’s status as a nonpsychoactive, well-tolerated therapeutic compound.
Routine follow-ups, adherence checks, and patient diaries confirmed strong compliance and high acceptability of CBD among participants. This supports its feasibility for integration into long-term treatment.
Clinical implications and broader therapeutic perspective
The current study evidenced that CBD, when used in conjunction with the ongoing levodopa therapy, can efficiently manage the PD symptoms, particularly those that are previously inadequately addressed by dopaminergic drugs. The efficacy can be monitored in motor and nonmotor symptoms. Additionally, the potential interaction with protein intake suggests that personalized nutritional planning could further optimize outcomes.
Similarly, the chronic nature of PD and the progressive decline associated with long-term levodopa monotherapy and the integration of phytotherapeutic compounds like CBD offer a multifaceted strategy for symptom control and possibly disease modification. These findings pave the way for more robust, long-term clinical trials with larger cohorts and biomarker analyses to validate the observed effects and elucidate the molecular pathways involved. Additionally, future studies could explore CBD’s potential neuroprotective roles and its capacity to delay disease progression, beyond mere symptomatic relief.
Our findings further elucidated the role of dietary protein in modulating CBD’s efficacy. While CBD demonstrated significant improvements across various motor and nonmotor symptoms independently (e.g., as shown by average UPDRS score improvements in sensory complaints related to Parkinsonism (1.92), tremor (1.88), and walking and balance (1.83) in the CBD group, the synergistic effect was notable when CBD was administered alongside protein supplementation. For instance, in the CBD with protein group, the average improvement in sensory complaints related to Parkinsonism was 2.25, turning in bed was 2.21, and tremor was 2.08. These results suggest that while CBD is effective alone, a personalized dietary approach incorporating protein could potentially optimize therapeutic outcomes, especially for specific symptoms like turning in bed and tremors. It is critical to consider the well-established impact of dietary protein on levodopa absorption in PD management. Large neutral amino acids (LNAAs) present in protein-rich foods compete with levodopa for transport across the intestinal lumen and the blood–brain barrier. This competition can lead to fluctuations in levodopa plasma levels and reduced central nervous system availability, potentially causing motor complications. Therefore, while our study highlights CBD’s adjunctive benefits, careful dietary planning regarding protein intake is crucial to maximize levodopa’s therapeutic window and prevent motor fluctuations, alongside exploring synergistic effects with compounds like CBD.
Conclusion and Recommendations
Conclusion
This study demonstrated that CBD, when used alongside levodopa, offers a meaningful enhancement in both motor and nonmotor symptom control in PD. Notably, the integration of dietary protein timing further amplifies therapeutic gains, underscoring the importance of a multidimensional approach to PD management. As one of the first randomized trials to explore this triad of CBD, levodopa, and protein modulation, the findings provide a compelling foundation for rethinking adjunctive strategies in PD care. Given the favorable safety profile of CBD and its capacity to address symptoms unresponsive to conventional therapies, this research supports its consideration as part of future integrated treatment protocols. Large-scale trials are warranted to validate these results and explore long-term neuroprotective potentials.
Recommendations
Future research should focus on conducting larger, long-term randomized controlled trials to validate the sustained efficacy and safety of CBD as an adjunctive therapy in PD, alongside exploring optimal dosing strategies and formulations. Integrating biomarker analysis in these trials is crucial in objectively confirming symptomatic improvements and elucidating underlying neurobiological mechanisms. Furthermore, continued investigation into refined personalized nutritional strategies, particularly concerning dietary protein and its interaction with CBD and levodopa, is recommended to optimize therapeutic outcomes. Finally, delving into CBD’s potential neuroprotective effects beyond symptomatic relief should be a key area of future inquiry to assess its capacity for disease modification.
Limitations of the study
This study, though promising, has several limitations. First, the relatively small sample size of 96 participants and the 8-week intervention period limit the generalizability and long-term assessment of CBD’s efficacy and safety in PD. Second, though dietary protein was controlled, detailed pharmacokinetic analyses of CBD or levodopa to protein timing were not conducted, thus precluding a precise mechanistic understanding of their interaction. Future research should address these limitations through larger, long-term trials incorporating comprehensive pharmacokinetic studies and objective biomarker analyses to further validate and optimize CBD as an adjunctive therapy for PD.
Availability of data and materials
All the data generated in this research work has been included in the manuscript.
Acknowledgment
The authors are thankful to Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2025R419), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Author Contributions
Conceptualization, Afia Zia; methodology, Wajid Rahim Awan; software, Niamat Ullah; validation, Ammena Y. Binsaleh and Nawal Al-Hoshani; formal analysis, Adnan Khan; investigation, Wajid Rahim Awan and Adnan Khan; resources, Afia Zia; data curation, Abdullah A. Alqasem; writing—original draft preparation, Wajid Rahim Awan and Adnan Khan; writing—review and editing, Reham M. Mashat; visualization, Ibrahim Faisal Halawani and Majid Alhomrani; supervision, Afia Zia.; project administration, Afia Zia; funding acquisition, Afia Zia
Conflicts of Interest
The authors declare no conflict of interest.
REFERENCES
Ajagun, E.J., Asuku, A.O., Ayinla, M.T., Abdulsalam, T.A., Ajibare, A.J., Olajide, T.S., et al. 2024. Pharmacotherapy of Parkinson’s disease and their limitations. In: Mohamed, W., editor. Zebrafish as a model for Parkinson’s disease. Boca Raton: CRC Press. pp. 186–203.
Behl, T., Kaur, G., Bungau, S., Jhanji, R., Kumar, A., Mehta, V., et al. 2020. Distinctive evidence involved in the role of endocannabinoid signalling in Parkinson’s disease: A perspective on associated therapeutic interventions. International Journal of Molecular Sciences. 21(17): 6235. 10.3390/ijms21176235
Belgers, V., Röttgering, J.G., Douw, L., Klein, M., Ket, J.C., van de Ven, P.M., et al. 2023. Cannabinoids to improve health-related quality of life in patients with neurological or oncological disease: A meta-analysis. Cannabis and Cannabinoid Research. 8(1): 41–55. 10.1089/can.2021.0187
Ben-Shlomo, Y., Darweesh, S., Llibre-Guerra, J., Marras, C., San Luciano, M., and Tanner, C., 2024. The epidemiology of Parkinson’s disease. The Lancet. 403(10423): 283–292. 10.1016/S0140-6736(23)01419-8
Bhunia, S., Kolishetti, N., Arias, A.Y., Vashist, A., and Nair, M., 2022. Cannabidiol for neurodegenerative disorders: A comprehensive review. Frontiers in Pharmacology. 13: 989717. 10.3389/fphar.2022.989717
Chagas, M.H.N., Zuardi, A.W., Tumas, V., Pena-Pereira, M.A., Sobreira, E.T., Bergamaschi, M.M., et al. 2014. Effects of cannabidiol in the treatment of patients with Parkinson’s disease: An exploratory double-blind trial. Journal of Psychopharmacology. 28(11): 1088–1098. 10.1177/0269881114550355
Dach, J., Moore, E.A., and Kander, J., 2015. Cannabis extracts in medicine: The promise of benefits in seizure disorders, cancer and other conditions. Jefferson, NC: McFarland.
Dalla Verde, C., Jayanti, S., El Kobar, K., Stanford, J.A., Tiribelli, C., and Gazzin, S., 2025. Understanding the pre-clinical stages of Parkinson’s disease: Where are we in clinical and research settings? International Journal of Molecular Sciences. 26(14): 6881. 10.3390/ijms26146881
De Meijer, E.P.M., 2009. Cannabinoid profiling of Cannabis samples for purity analysis. Journal of Natural Products.
Del-Bel, E., de Souza Lisbôa, S.F., and Gomes, F.V., 2024. Cannabidiol in neurology and psychiatry. Oxford: Elsevier. Vol. 177.
Ferrer, I., 2011. Neuropathology and neurochemistry of nonmotor symptoms in Parkinson’s disease. Parkinson’s Disease. 2011(1): 708404. 10.4061/2011/708404
Flores-Sanchez, I. J., and Verpoorte, R., 2008. PKS activities and biosynthesis of cannabinoids and flavonoids in Cannabis sativa L. plants. Plant and Cell Physiology. 49(12): 1767–1782. 10.1093/pcp/pcn150
Grotewold, N., and Albin, R.L., 2024. Update: Descriptive epidemiology of Parkinson’s disease. Parkinsonism & Related Disorders. 120: 106000. 10.1016/j.parkreldis.2024.106000
Hazekamp, A., 2008. Review: Cannabis—From cultivar to chemovar. Drug Testing and Analysis. 4(7–8): 660–667. 10.1002/dta.407
Hodgson, P., Jordan, A., Sinani, C., and Charura, D., 2025. Examining the relationship between physical function and anxiety/depression in Parkinson’s. Brain and Behavior. 15(5): e70563. 10.1002/brb3.70563
Jiang, Y., Qi, Z., Zhu, H., Shen, K., Liu, R., Fang, C., et al. 2025. Role of the globus pallidus in motor and non-motor symptoms of Parkinson’s disease. Neural Regeneration Research. 20(6): 1628–1643. 10.4103/NRR.NRR-D-23-01660
Khor, S.P., and Hsu, A., 2007. The pharmacokinetics and pharmacodynamics of levodopa in the treatment of Parkinson’s disease. Current Clinical Pharmacology. 2(3): 234–243. 10.2174/157488407781668802
Kumar, L., Malhotra, M., Singh, A.P., and Singh, A.P., 2024. Comprehensive review on Parkinson’s disease: Insights into prevalence, pathophysiology, diagnosis, and multifaceted treatment approaches. Journal of Drug Delivery & Therapeutics. 14(6): 200–213. 10.22270/jddt.v14i6.6637
Müller, T., 2020. Pharmacokinetics and pharmacodynamics of levodopa/carbidopa cotherapies for Parkinson’s disease. Expert Opinion on Drug Metabolism & Toxicology. 16(5): 403–414. 10.1080/17425255.2020.1750596
Müller, T., 2025. Clinical pharmacokinetics of levodopa and relevant add-on therapies for Parkinson’s disease. Expert Opinion on Drug Metabolism & Toxicology. 21(3): 279–288. 10.1080/17425255.2024.2428831
Müller, T., Gerlach, M., Hefner, G., Hiemke, C., Jost, W.H., and Riederer, P., 2024. Therapeutic drug monitoring in Parkinson’s disease. Journal of Neural Transmission. 131(10): 1247–1262. 10.1007/s00702-024-02828-5
Nord, M., 2017. Levodopa pharmacokinetics-from stomach to brain: A study on patients with Parkinson’s disease. Vol. 1567. Medical Dissertation. Department of Clinical and Experimental Medicine, Linköping University, Sweden.
Omotayo, O.P., Lemmer, Y., and Mason, S., 2024. A narrative review of the therapeutic and remedial prospects of cannabidiol with emphasis on neurological and neuropsychiatric disorders. Journal of Cannabis Research. 6(1): 14. 10.1186/s42238-024-00222-2
Peña-Zelayeta, L., Delgado-Minjares, K., Rojas, M.V., León-Arcia, K., Santiago-Balmaseda, A., Andrade-Guerrero, J., et al. 2025. Non-motor symptoms in Parkinson’s disease. Journal of Personalized Medicine. 15(5): 172. 10.20944/preprints202503.1395.v1
Rana, A.Q., Ahmed, U.S., Chaudry, Z.M., and Vasan, S., 2015. Parkinson’s disease: A review of non-motor symptoms. Expert Review of Neurotherapeutics. 15(5): 549–562. 10.1586/14737175.2015.1038244
Riederer, P., Strobel, S., Nagatsu, T., Watanabe, H., Chen, X., Löschmann, P.A., et al. 2025. Levodopa treatment: Impacts and mechanisms throughout Parkinson’s disease progression. Journal of Neural Transmission (Vienna). 132(6): 743–779. 10.1007/s00702-025-02893-4
Rinaldi, D., 2025. Motor and non-motor symptoms in advanced Parkinson’s disease: Current insights and future directions. Doctoral Thesis. Università degli Studi di Roma La Sapienza.
Rusch, C., Flanagan, R., Suh, H., and Subramanian, I., 2023. To restrict or not to restrict? Practical considerations for optimizing dietary protein interactions on levodopa absorption in Parkinson’s disease. NPJ Parkinson’s Disease. 9(1): 98. 10.1038/s41531-023-00541-w
Schneider, S.A., and Obeso, J.A., 2014. Clinical and pathological features of Parkinson’s disease. Current Topics in Behavioral Neurosciences. 22: 205–220. 10.1007/7854_2014_317
Su, D., Cui, Y., He, C., Yin, P., Bai, R., Zhu, J., et al. 2025. Projections for prevalence of Parkinson’s disease and its driving factors in 195 countries and territories to 2050: Modelling study of Global Burden of Disease Study 2021. BMJ. 388: e080952. 10.1136/bmj-2024-080952
Suryadevara, U., Bruijnzeel, D.M., Nuthi, M., Jagnarine, D.A., Tandon, R., and Bruijnzeel, A.W., 2017. Pros and cons of medical cannabis use by people with chronic brain disorders. Current Neuropharmacology. 15(6): 800–814. 10.2174/1570159X14666161101095325
Tambasco, N., Romoli, M., and Calabresi, P., 2018. Levodopa in Parkinson’s disease: Current status and future developments. Current Neuropharmacology. 16(8): 1239–1252. 10.2174/1570159X15666170510143821
Teil, M., Al-Kassmy, J., Alsalmi, M., Al-Rawahi, B., and Huot, P., 2025. The on-going quest for a long-acting oral form of levodopa. Expert Opinion on Drug Metabolism & Toxicology. 20: 1–10. 10.1080/17425255.2025.2535177
Vimal, D., D’Souza, L.C., Rai, V., Lal, S., Sharma, A., and Gupta, S.C., 2023. Efficacy of cannabis and its constituents in disease management: Insights from clinical studies. Current Medicinal Chemistry. 30(2): 178–202. 10.2174/0929867329666220525124818
Wang, M., Wang, Y.-H., Wang, B., Avula, M.M., Radwan, A.S., Wanas, J., et al. 2017. Decarboxylation study of acidic cannabinoids: A novel approach using ultra-high-performance supercritical fluid chromatography/photodiode array–mass spectrometry. Cannabis and Cannabinoid Research. 2(1): 1–11. 10.1089/can.2016.0020